The amount is substantial, representing a decrease by a third from 2018 (when it received 106 B).
The cuts have received substantial criticism, even from the President’s own allies – most notably, the House Appropriations Committee Chairman and Davao City First District Representative Karlo Nograles. News articles about the cuts tell us little about where the cuts are and what it actually means for health service delivery. At best, the articles mention deep cuts to the Health Facility Enhancement Program (HFEP) and the health human resources deployment programs (such as the Doctors to the Barrios (DTTB) Program).
The cuts are contrary to the government’s populist agenda. This is the government that passed free tuition for all public universities, a comprehensive tax reform law that lowered personal income tax, and free irrigation to farmers owning less than 8 hectares of land. The House version of the Universal Health Coverage (UHC) Bill, the country’s most ambitious health reform legislation ever, passed with an overwhelming majority (222-7-0), and everyone is hopeful that the Senate would pass their version soon. Duterte also urged Congress to pass the UHC Bill immediately in his last State of the Nation Address.
How does one reconcile Duterte’s promises of universal health coverage and the budget cuts to the Department of Health (DOH)? The situation is definitely more nuanced than what is reported in the media, and publicly available information can readily explain these cuts.
We start by looking closely at the Department of Budget and Management’s (DBM) National Expenditure Program (NEP). The NEP is the annual budget document prepared by the executive branch and serves as the starting point for deliberations of the budget, officially known as the General Appropriations Act (GAA), in Congress. The full documents are available in the DBM website.
The DOH NEP is broken down into 8 programs, the names of which are not known to most people (the program classifications are not intuitive – what most people know are the subprogams to these general program categories). Without adjusting for inflation, we can summarize the percent changes of the appropriations per program from 2018 to 2019.
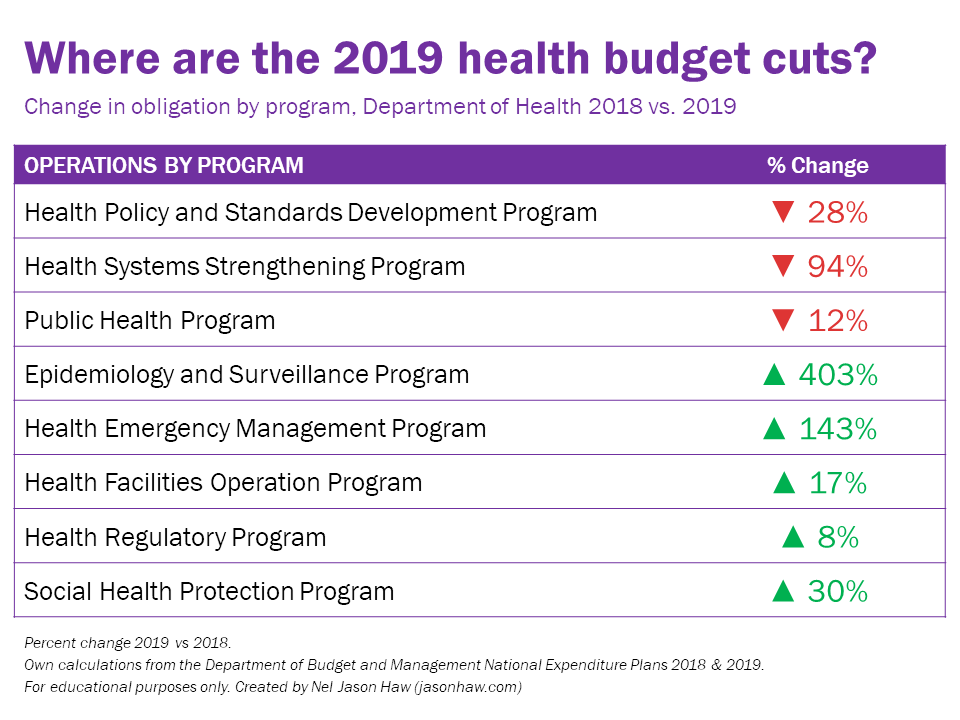
Five out of the eight programs actually received significant increases. Most notable increases are in three programs: the Epidemiology and Surveillance Program, Health Emergency Management Program, and the Social Health Protection Program.
The Epidemiology and Surveillance Program has a five-fold increase because of the 217 M special allocation for the surveillance of the 800,000-plus children who were vaccinated with Dengvaxia (see DBM’s official release here, page 26). This is the government’s guarantee that resources will be allocated to properly monitor the health outcomes of these children.
The Health Emergency Management Program is receiving an additional 500 M as a Quick Response Fund (QRF). QRFs are standby funds that can readily be used by government agencies whenever a disaster strikes, and the disbursement does not require approval by the National Disaster Risk Reduction and Management Council (NDRRMC). Five agencies are already receiving QRFs, and in 2019, the national government wants to add DOH to its list of recipients. After all, DOH needs to respond when natural and man-made disasters strike, particularly health-specific events like epidemics.
The Social Health Protection Program is a discretionary fund that DOH uses in providing direct financial assistance to indigent patients, on top of the support that the Philippine Health Insurance Corporation (PhilHealth) already guarantees as part of its No Balance Billing (NBB) scheme, and support from other agencies such as the Philippine Charity Sweepstakes Office (PCSO) and Department of Social Welfare and Development (DSWD). The fund will receive an additional 1 B from 2018.
The budget cuts mentioned in news articles pertain specifically to the Health Systems Strengthening Program. Under this program are both HFEP and the human health resources deployment programs.
HFEP is a DOH program aimed at building and rehabilitating health facilities both managed by the national government and local government units (LGUs) (Unlike public schools, management of health facilities are devolved to LGUs, save for around 70 public teaching hospitals). The fund received substantial increases upon the passage of the Sin Tax Law in 2012. While 80% of the 85% of the sin tax revenues earmarked for health are being used to subsidize the PhilHealth premiums of indigent families, the remainder is appended to the DOH budget. A simple time trend analysis of the budget obligations of HFEP shows how rapid the increases in allocation were:
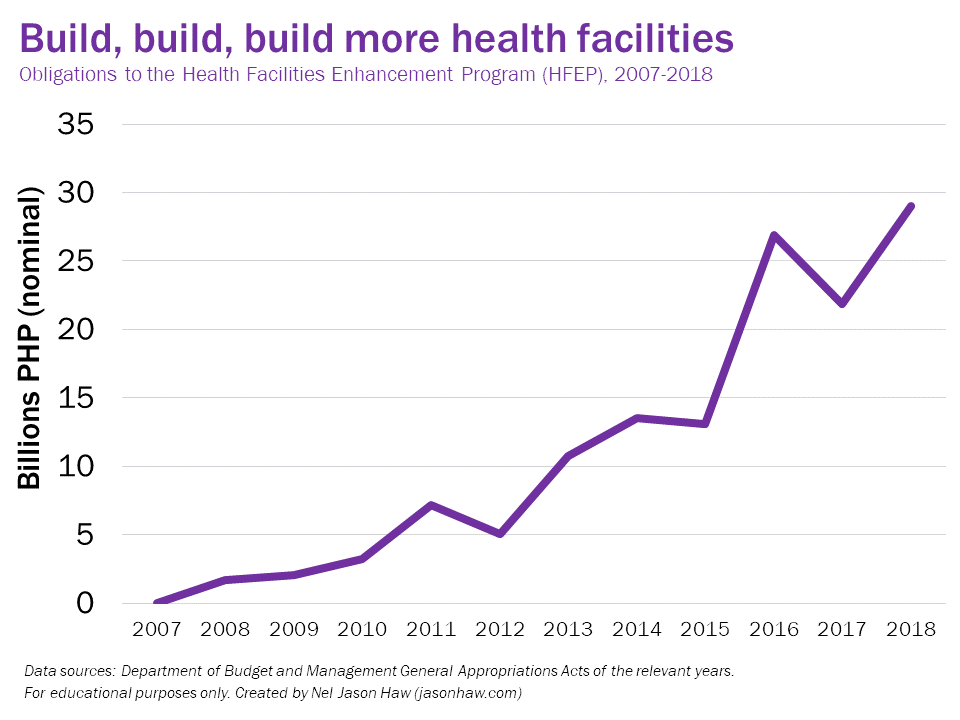
In 2019, HFEP is virtually eliminated – only 50 M as compared to the 30 B it received in 2018. There are two related reasons for this drastic cut. First, the spending performance of HFEP has been poor. DBM has been explicit about its criticism of HFEP (a detailed analysis can be found here). As a result, DOH’s budget utilization rate (BUR) has always been less than 90%, far lower than the 100% target set by DBM. Second, the government wants to shift from obligation-based budgeting to cash-based budgeting for 2019. This shift requires appropriations that are only “shovel-ready,” meaning that a government agency should be ready to disburse the funds in the same year that they are appropriated. In obligation-based budgeting, funds can be disbursed for up to two years after it was appropriated, resulting to delays in disbursement and chronic underspending of many government agencies. As a result, DBM wants DOH to fulfill all of its disbursements in previous appropriations and implement the corresponding projects, before it will propose to Congress for another set of appropriations. Assuming DOH does this and DBM keeps its word, this budget cut is only temporary.
The issue of health human resource deployment programs has something to do with the way the budget has been appropriated in previous years. A closer look at the 2018 vs. 2019 budget for this particular subprogram presents a curious case:
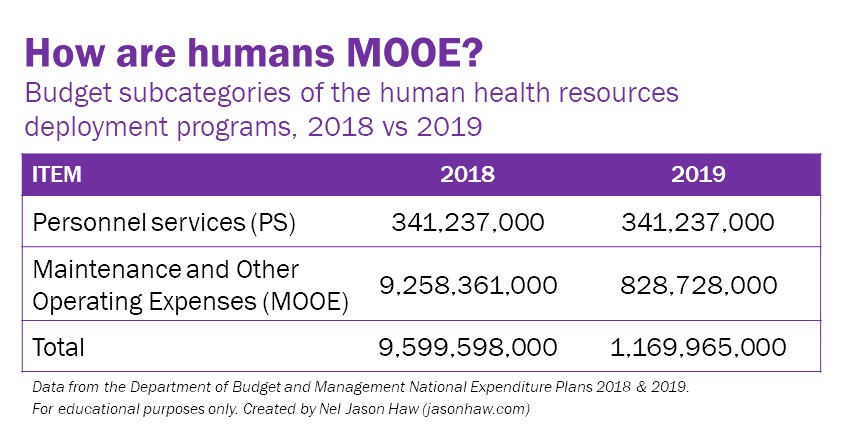
Personnel services (PS) remained the same between 2018 and 2019, and the cuts are isolated in the maintenance and other operating expenses (MOOE). Since this is a program that largely involves salaries to health professionals, why is the MOOE share much larger? This is because most allied health professionals like nurses are not counted as personnel. They are counted as contractual employees or job orders, or more commonly known as “endo.” Last May, the President signed Executive Order 51, effectively ending the practice of “endo” in all government agencies. This means that government agencies must either provide security of tenure to previously contractual staff or refuse to hire contractual employees again. The DOH took the latter approach, citing concerns about the civil service eligibility of most allied health professionals. This was mentioned explicitly by Health Secretary Francisco Duque III during the DOH budget interpellations at the House last September 3. DOH is now proposing a compromise solution, where these health professionals will still be considered contractual employees but will be provided government-mandated benefits so that their line item now becomes PS instead of MOOE.
As of posting this article, the 2019 GAA is still being deliberated. This means that the final budget cuts to DOH are still unknown, but understanding how the budget was proposed originally in the NEP gives us a perspective on how the government is trying to be more effective in its duties. While this budget cut can easily shock anyone at first glance, it is important for us to understand how much more nuanced the situation is, and that we can use publicly available sources to paint a clearer picture of the context behind this.
Links to sources and further reading are cited in-text.
